Thyroid School, Issue #23// Gut Health + Thyroid, Introduction
January 30th, 2023
Gut Overview
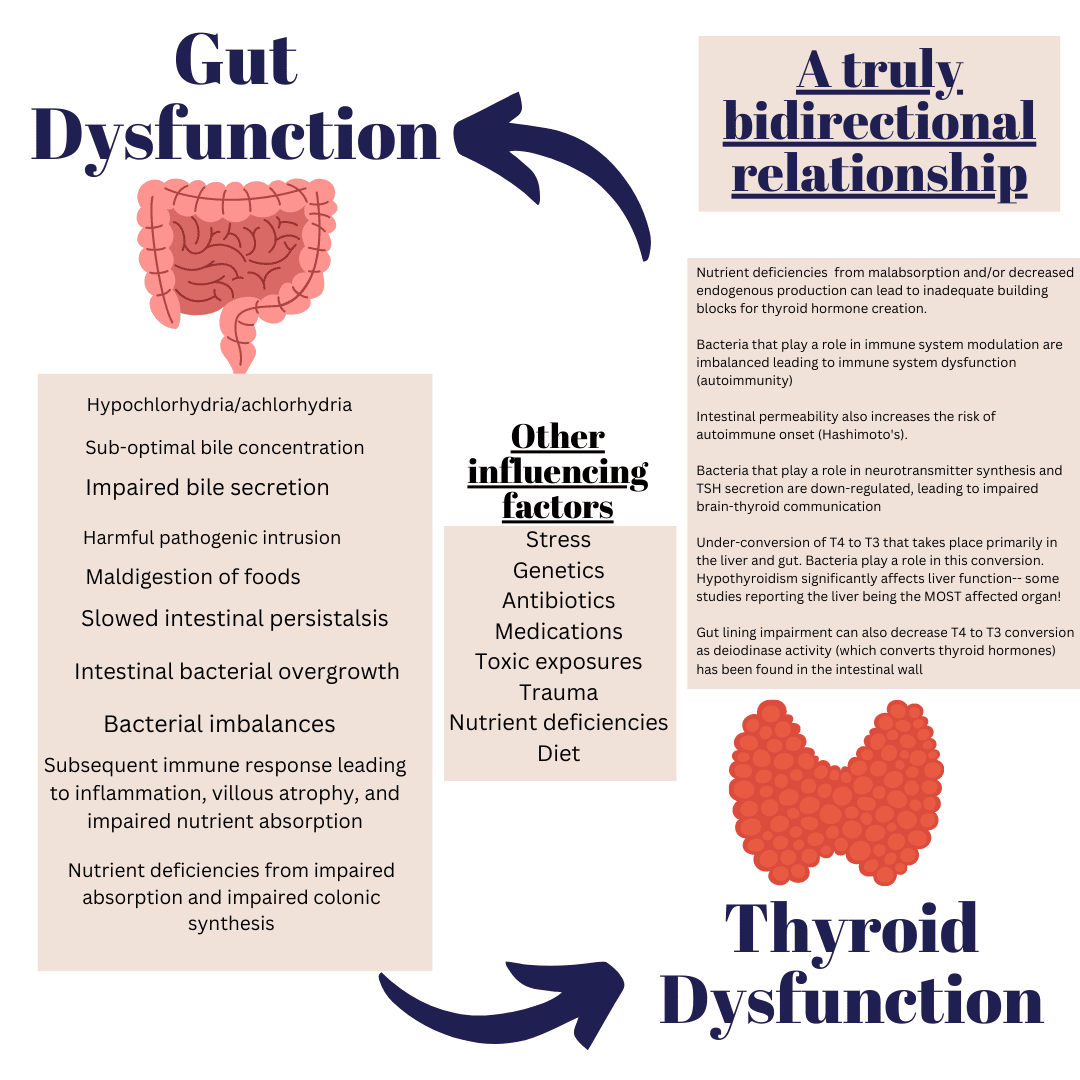
Thyroid hormones are the pacesetters of the body— from metabolic rate the intestinal peristalsis rate. Many who have thyroid dysfunction complain in some way of gastrointestinal symptoms, but the connection between thyroid and gut are rarely discussed and often treated as separate issues, when in fact there is an intimate relationship.
Thyroid hormones affect nearly every aspect of gastrointestinal function, and the GI tract affects thyroid function. It is a classic example of “chicken or egg” in which each person’s root cause(s) differ from the next.
Appreciating the impact that thyroid hormones have on each step of the digestive process magnifies just how hypothyroidism leads to a host of symptoms. Thyroid integrity is the rate limiting step in an orchestra of metabolic functions that has cascading effects when even the slightest bit off. Deviations from “normal” can lead to a snowball of events that creates a cycle of GI distress, intestinal alterations, and rebound thyroid hormone disruption that perpetuates this cycle.
Hypothyroidism has been shown to be linked to autoimmunity in 95% of cases. Hashimoto’s is most common in women between the ages of 30-50 years old and impacts women 10x more than men. Genetic predisposition plays a role in the development of autoimmune thyroid disorders, like Hashimoto’s, but also includes other possible triggers like:
Excessive iodine intake (more common in Hashimoto’s), but also inadequate iodine intake (mostly in non-autoimmune situations)
Nutrient deficiency (zinc, Vitamin D, selenium, iron, glutathione, and more)
Infections (H. Pylori, Yersinia, Epstein- Barr Virus (EBV), Hepatitis C, and even enteroviruses (stomach “bugs”)
Stress and trauma (with studies showing that 80% of those with Hashimoto’s have a major stressor or traumatic event leading up to their diagnosis)
In regards to the GI tract, those with Hashimoto’s are more likely to have:
Anti-parietal cell antibodies (APCA): antibodies against the parietal cells; parietal cells play a major role in gastric acid secretion and B12 absorption. Low parietal cell function can be a reason for B12 deficiency and impaired digestion leading to gas, bloating, indigestion, irregular bowel movements, and even high risk of SIBO (see below)
SIBO (small intestinal bacterial overgrowth): occurs when there is an overgrowth of bacteria in the small intestines that can lead to gas, bloating, diarrhea, constipation, nutrient deficiencies, and more. It can be both a cause and effect of thyroid dysfunction. SIBO can occur due to slow transit time of the gut, bacterial invasion from low defense systems (such as low stomach acid), repeated vomiting, constipation, and more.
H. Pylori: a bacteria that resides in the stomach that, when overgrown, can affect stomach acid secretion, digestion, and be a big risk factor for the development of Hashimoto’s.
IBS (irritable bowel syndrome) is a diagnosis by exclusion (which means that other bowel disease have been ruled out). IBS can be caused by bacterial imbalances, poor digestive enzyme production, slow or fast motility, and more.
Celiac disease: an autoimmune disease in which the immune system reactions to the ingestion of gluten containing grains. This is one of the most common co-morbidities in those with Hashimoto’s.
Inflammatory bowel disease (IBD) is a term for two conditions (Crohn’s disease and Ulcerative Colitis) that are characterized by chronic inflammation of the gastrointestinal (GI) tract. Prolonged inflammation results in damage to the GI tract.
The gut microbiome is a complex system of symbiotic organism made up of mostly bacteria, with estimates around a trillion or more bacteria residing in the human GI tract at any given point. You actually have more bacterial cells in your body than human cells!
But before we start talking bacteria, let’s start from the top and work out way down the gastrointestinal tract digestive process and see where thyroid hormones play a role:
Mouth: thyroid hormones affect the release of saliva from salivary glands. Studies show up to 50% of patients with hypothyroidism experience low saliva production which can impair chewing and swallowing. Beyond that, those with AITD (autoimmune thyroid disease) are at increased risk of other autoimmune diseases like Sjögren’s syndrome in which the salivary glands are affected. Low salivary output can also affect the oral microbiome (bacterial levels) leading to cavities, bad breath, mouth sores, gum disease, and dry mouth/lips.
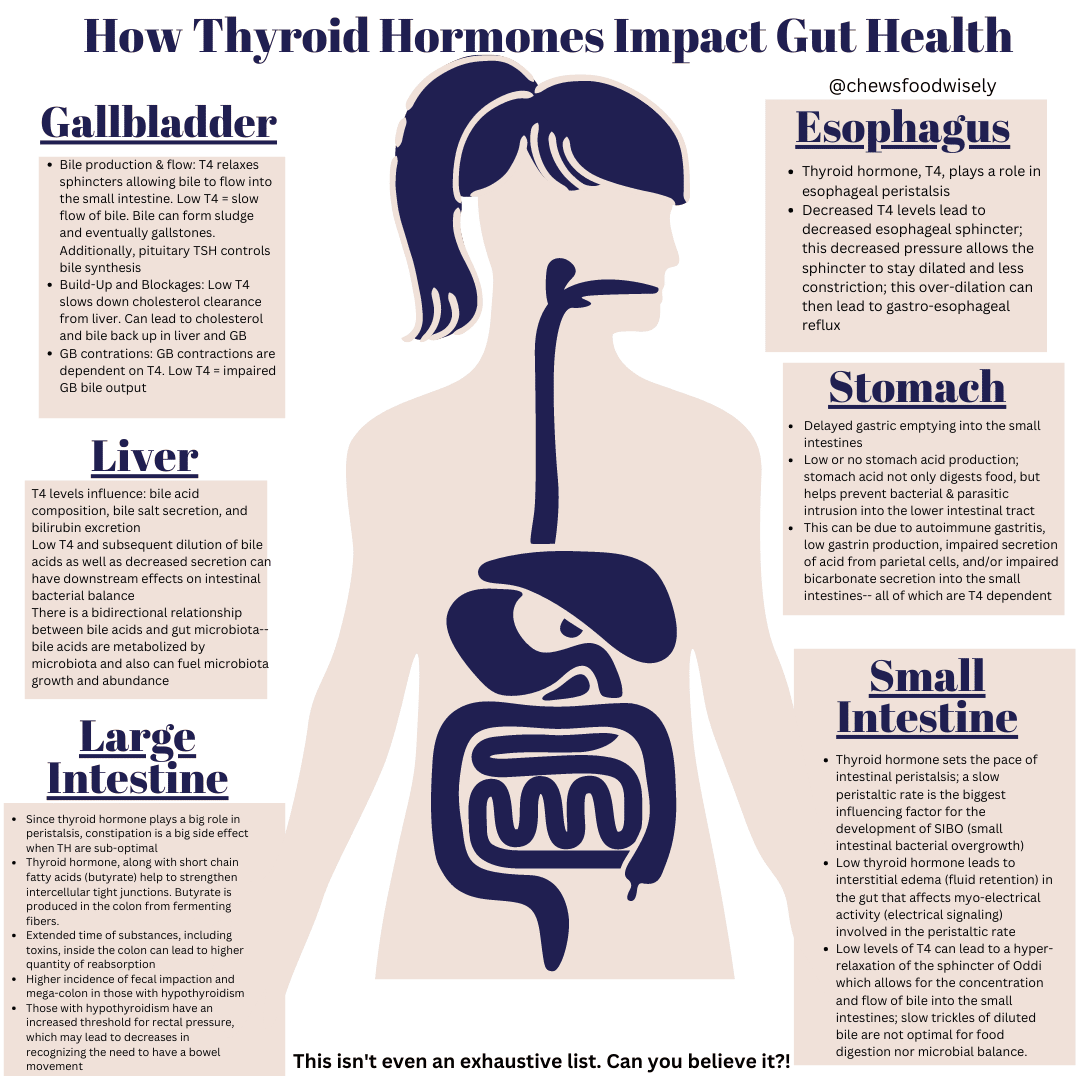
Esophagus: thyroid hormones help to maintain cellular tone and low levels can lead to edema in the interstitial muscle later in the intestines. This fluid build up, called edema, blocks electrical signaling that drives peristalsis (or the contraction of the intestinal tract— including the esophagus). A decrease in this myo-electrial (myo=muscular) activity causes low esophageal sphincter pressure which causes the esophageal sphincter to stay open longer than it should. Because the sphincter isn’t closing property, food and acid from the stomach can regurgitate into the esophagus causing “reflux” symptoms.
Stomach: thyroid hormones also play a role in gastric emptying as well as the production of stomach acid. Low stomach acid combined with decreased speed of stomach emptying allows food to sit in the stomach longer than it should which leads to fullness and gas. This also contributes to reflux. Additionally, thyroid hormones help produce hydrochloric acid and those with Hashimoto’s are at increased risk of APCA (anti-parietal cell antibodies) which can affect stomach acid production.
Liver & Gallbladder: thyroid hormones help with the production of bile from cholesterol as well as the recycling of bile acids to create secondary bile acids. Thyroid hormones regulate the rate of production of bile acids as well as the flow of bile from the liver, to the gallbladder, and into the intestinal tract. Low levels of T4 hormone causes a hyper-relaxation of the sphincter of Oddi in the gallbladder which impairs the concentration of bile and affects how well the bile is able to perform on digestion.
Intestinal tract (small intestines & colon): thyroid hormones help to trigger peristalsis of the intestinal tract, so low levels will lead to slowing of the intestinal contractions. Slow transit time is one of the leading causes of SIBO (small intestinal bacterial overgrowth) which can cause impaired digestion, decreased nutrient absorption, and symptoms such as bloating, gas, diarrhea, and constipation. Those with hypothyroidism are at increased risk for constipation, ileus, and pseudo-obstruction. Additionally, hypothyroid patients have been documented to have enlarged tight junctions and thicker, shorter villa and micro-villi. Thyroid hormones help with gastrointestinal development and help promote tolerance to commensal (or “good”) bacteria. Thyroid hormones help to create homeostasis in the intestinal epithelium via the interaction between T3 and thyroid hormone receptors present in the intestinal wall. Additionally, thyroid hormones, specifically T3, help to preserve gut microbiota by supporting an enzyme called IAP, which is a brush border enzyme secreted by the intestinal epithelium that acts as a defense system for the gut mucosa. It helps to prevent translocation of LPS (lipopolysaccharides) into circulation. LPS are hard outer membranes of “bad” bacteria that can trigger the immune system and create inflammation.
Now that we’ve covered SOME of the thyroid-gut interaction, the biggest question: which came first? Gut imbalance or thyroid imbalance?
The answer… it depends!
While thyroid hormones impact the gut, the opposite is true in that the gut impacts practically every level of endogenous (internal) and exogenous (externally introduced) levels of circulating levels of thyroid hormones via several mechanisms including:
impact on brain activity (including the stimulation of pituitary gland secretion of TSH)
immune function (especially important for those with autoimmunity)
absorption of nutrients necessary to create thyroid hormones
absorption and utilization of medication
entero-hepatic (intestinal/liver) recycling of medication
endogenous (or internal) regulation of thyroid hormones via microbiota “pooling” of hormones (AKA a safety reserve of thyroid hormones in the gut)
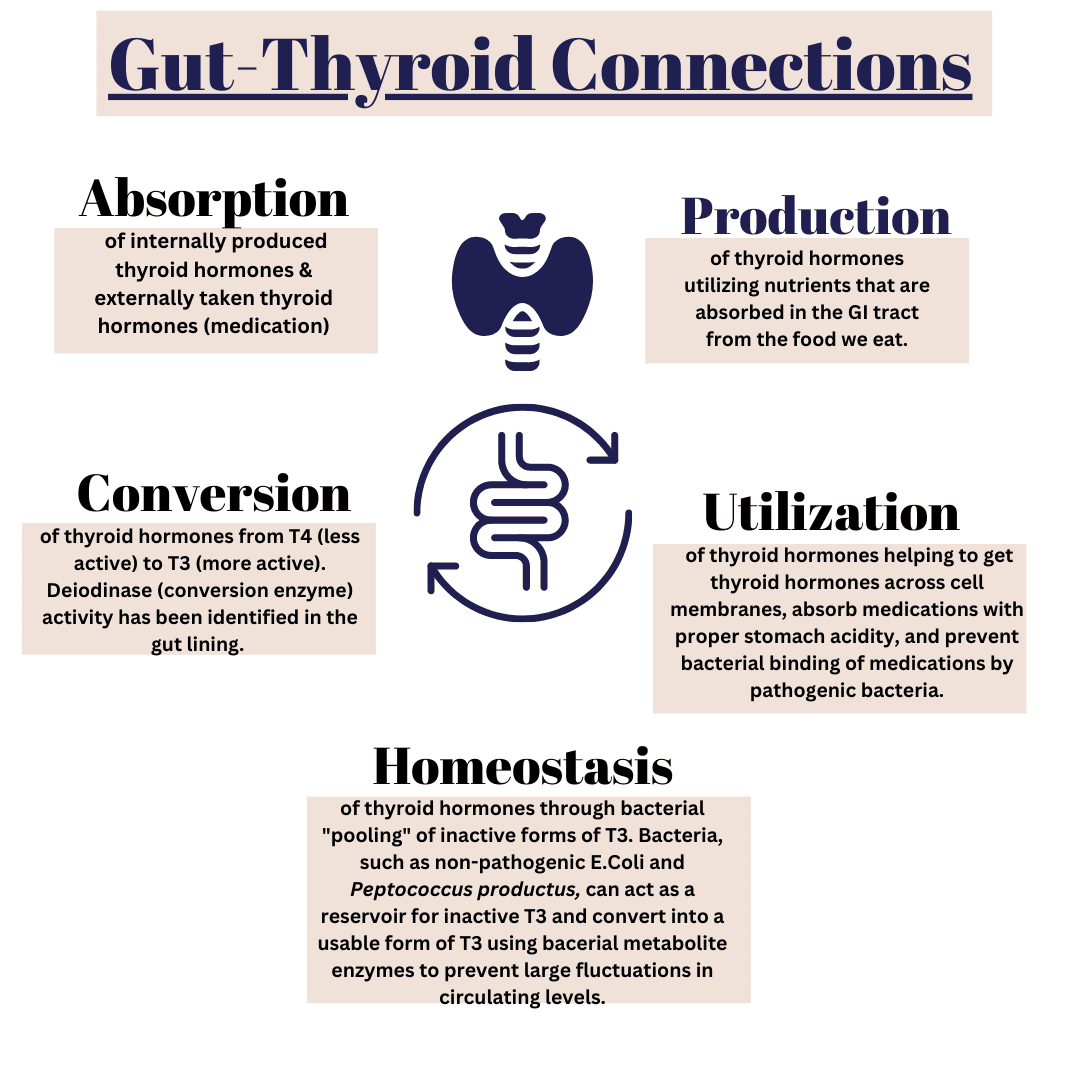
To organize it, thyroid-gut connections appears to be significant for a few primary reasons:
1. Absorption
Inflammation in gut lining prevents absorption
Opportunistic and pathogenic bacteria binding to thyroid hormones making them unusable
2. Production of thyroid hormones
Nutrient deficiencies leading to low levels of thyroid hormone building blocks
Impaired neurotransmitter creation impacting hypothalamic-pituitary signaling. When the brain doesn’t signal the thyroid, the thyroid won’t release hormones
Autoimmune activity leading to thyroid gland destruction and impairing thyroid hormone output. Gut integrity is paramount to autoimmune disease management given that 70% of the immune system is inside the GI tract!
3. Conversion
Deiodinase (D2) activity in gut lining. Deiodinases help covert T4 to T3 (inactive to active thyroid)
Conversion of T4 to T3 is also nutrient dependent and poor gut integrity can lead to nutritional deficiencies. More specifically, bacteria help with the absorption of minerals like zinc and selenium which are imperative for the thyroid conversion.
4. Utilization of thyroid hormones
The entero-hepatic (intestinal, liver) recycling of T4 medication affects how well the body utilizes medications
Absorption of medication requires adequate stomach acidity. Those on PPI and/or with history of low stomach acid often require higher medication dosing.
Pathogenic and opportunistic bacteria, like H. Pylori, can bind to medication and decrease the efficacy of them requiring higher dosing.
5. Homeostasis of thyroid hormones
Bacteria, like non-pathogenic E.Coli and Peptococcus productus, can act as a reservoir for T3 and prevent large fluctuations in levels. In other words, these bacteria can absorb the “inactive” T3 and then release and convert to a more active form with enzymes like beta-glucuronidase. Beta-glucuronidases and bacterial sulfatases, both microbial enzymes, help to turn a less active form of T3 into a more active form of T3 in a process called “iodothyronine deconjugation”.
The biggest influences to the above list include:
Microbial balance (aka bacterial balance)
Immuno-modulation
Preventing pathogenic infiltration
Supporting immune system due to “good bacteria’s” immune-modulating properties
Production of metabolites:
SCFA// short chain fatty acids (butyrate, propionate, acetate)
Motility & movement of matter through the GI tract; this also include the MMC (migrating motor complex).
Bacteria:
Bacterial levels are a delicate balance and can be influenced by several factors including, but not limited to:
Route of birth (with vaginally born babies expressing higher diversity versus those born Cesarean)
Means of feedings as baby (breast versus formula)
Exposures to medications throughout life (antibiotics, antacids, NSAIDS, steroids, etc.)
Stress (as stress hormones can alter intestinal lining integrity and affect peristaltic rate)
Trauma
Diet (more on this later!)
Nutrient levels
Alcohol & drug use
Toxic exposure (pesticides, pollution)
Nutritionally speaking, one of the best predictors of good health is the inclusion and diversification of fibers. The fermentation of fibers help with the production of several compounds including:
Short Chain Fatty Acids (SCFA): butyrate, propionate, and acetate
Leptin helps to regulate appetite and food intake and helps to also stimulate the release of hypothalamic hormones (which then trigger TSH production from the pituitary gland. Leptin mediates cross-talk between adipose tissue (fat) and HPA-T axis (brain-adrenal-thyroid communication pathway).
GLP-1 (helps regulate insulin secretion and thus blood sugar levels)
Most bacteria resides in the large intestine, or colon, with the two dominant strains being Firmicutes and Bacteriodetes which account for approximately 90% of human bacteria. Bacteria help to modulate (regulate) both the innate and adaptive immune system inside and outside of the gut. This is significant to recognize that the immune system, which is estimated to be about 70% inside the GI tract, affects the entire body!
There are SO many things bacteria do, so I’ve compiled a list (which is not even an exhaustive list) of just SOME ways gut bacteria influence your thyroid status:
Influencing innate, cellular, and humoral immunity by interacting with epithelial and mucosal immune cells— especially important if you are predisposed or already have autoimmune disease.
Activate or inactive inflammatory and anti-inflammatory molecules. Inflamed gastrointestinal lining will impair nutrient and thyroid absorption, thus leading to nutrient deficiencies and possibly even thyroid hormone deficiency due to impaired absorption.
Affect thyroid hormone concentrations by controlling the uptake, degradation, and entero-hepatic (intestinal & liver) recycling of T4.
Good bacteria levels have been shown to lower TSH levels and decrease T4 dosing due to the impact on the immune system as well the digestive and absorptive capacity
Influence neurotransmitter production, including dopamine, which affects pituitary function and therefore TSH secretion;
Helps to produce SCFA (short-chain fatty acids) which, with the help of T3, maintains the strength and integrity of the gut lining and prevents gut permeability;
Influences secondary bile acids which regulate deiodinases, specifically D2. DIO2 is considered as primarily responsible for the local production of T3 inside cells and its presence has been detected in several locations, such as the pituitary gland and hypothalamus, cochlea, brown adipose tissue, bones, muscles, heart, and central nervous system.
Bacteria help with the digestion of food and absorption of nutrients. Therefore, imbalances of bacteria can hinder levels of nutrients available for the creation of thyroid hormones, distribution of them throughout the body, conversion of T4 to T3, and the absorption of thyroid hormones into the cell
low bacteria levels negatively affect immune function and lead to shortened villi, microvilli, and shallower crypts in the intestines which impairs nutrient absorption and increases permeability. More specifically, commensal bacteria help with the uptake of selenium, zinc, iodine, and iron— all of which affect production and conversion of thyroid hormones.
Decrease medication dosing (due to enhanced absorption of medication as well as conversion from T4 to T3)
Pathogenic and opportunistic bacteria have been shown to bind to thyroid hormones and prevent utilization and absorption
Decrease rates of depression, anxiety, brain fog (due to microbiota influences on neurotransmitter creation)
Decrease antibodies (due to the immuno-modulating effects of commensal bacteria)
Decrease TSH (again, due to the microbiota’s impact on neurotransmitter and eventually hypothalamic-pituitary function as well as the improved absorption and conversion of thyroid hormones)
Decreased inflammation (from both the direct impact on inflammatory and anti-inflammatory metabolites and the immune-modulating effects of probiotics)
Microbiota play a role in developing the GALT (gut associated lymphatic tissue) where approximately 70% of the immune system of the entire body resides. GALT is crucial for immune tolerance to “good” bacteria and food antigens while also eliminating potential harmful factors.
GALT helps with the development of tolerance to self-antigens (preventing the immune system from attacking “safe” objects in the body. Autoimmunity occurs when this is disrupted). The GALT is activated when the ability of the intestinal barrier to control transport of antigens is lost and immune cells from the intestinal tract migrate to tissues and cause inflammation from the immune system activation.
Bacterial metabolites (byproducts) including SCFA (short chain fatty acids), specifically butyrate, increase T-regulatory cells (which help to mediate and regulate the immune response) and decrease pro-inflammatory modules including TH-17.
SFCA help to strengthen tight junctions and prevent leaky gut. SCFA are anti-inflammatory and the primary fuel for the colonocytes (cells inside the colon/large intestine). The help with epithelial regeneration and repair, modulate lipid, hormone, and energy metabolism, improve tight junction integrity, can improve adhesion of intestinal cells, and decrease pH to protect against pathogens.
Bacterial imbalances and infections (including bacterial, viral, fungal, and parasitic) can stimulate an activation of the immune system which can lead to autoimmunity due to: molecular mimicry, epitope spreading, bystander activation, and presence of cryptic antigens.
Gut Lining:
a damaged gut lining leads to a penetration and exposure of pathogens to immune-reactive sub-epithleum which promised inflammation and autoimmune genesis
Studies consistently reveal increased levels of serum zonulin (a marker of gut permeability) and AITD (autoimmune thyroid disease)
deiodinase activity has been shown in the intestinal wall; inflammation and permeability affect the T4 to T3 conversion;
Bacteria modulate the expression of tight junctions, impact the shape of enterocytes, and the composition of mucous layer. Therefore, bacterial imbalances can lead to poor gut integrity and thus influence nutrient absorption, immune function, and eventually thyroid function;
Digestive Capacity:
– Hydrochloric Acid production: thyroid hormones help to regulate stomach acid secretion by altering the number and size of secretory cells inside the stomach. Those with autoimmune thyroid disorders are also more likely to have antibodies against the parietal cells inside the stomach which are responsible for acid production and release. Stomach acid is essential for thyroid medication absorption and studies show that those with low stomach acid or who take antacid medications require higher dosing of T4 medication. Hydrochloric acid in the stomach is one of the first line defenses against harmful pathogens (bacteria, viruses, parasites, etc.) from getting into the intestinal tract. Both too much and too little stomach acid yield similar symptoms, and in the case of hypothyroidism, symptoms are often related to too little stomach acid.
Primary & Secondary Bile Acids:
Thyroid hormones help to regulate the rate of bile acid synthesis as well as flow of bile acids from liver, into gallbladder, and into the intestinal tract
Secondary bile acids, initially triggered by thyroid hormones, impact energy metabolism by influencing insulin sensitivity and thus blood sugar regulation as well as activating D2 (the T4 to T3 enzyme).
Bile Acids:
Cholic Acid (CA)
Chenodeoxycholic Acid (CDCA)
Produced in the liver as a result of cholesterol metabolism via Cytochrome P450 pathway. Secreted into bile and helps with digestion along with bile salts
95% is reabsorbed in small intestines and 5% in colon
Via the microbiota (specifically bacteriodetes, eubacterium, bifidobacterium, ruminococcus, clostridia), they are converted via deconjugation and dehydroxylation into secondary bile acids:
Deoxycholic acid (DA)
Lithocholic acid (LA)
Ursodeoxycholic acid (UDCA)
Bile is anti-microbial and is another defense against pathogenic invasion. Bile helps with the digestion and emulsification of fats and is required for the digestion and integration of fat-soluble vitamins (like Vitamin A, D, E, K). Vitamin A and Vitamin D deficiency are risk factors for autoimmune disease.
You see, everything in the body is connected!!
Now, don’t let this overwhelm you. This is probably WAY more information than you’d like, but if you’re like me, you LOVE the nerdy, science stuff.
If you want the TLDR action steps, here you go:
Include a diverse array of fibers in your diet every day. Ideally, 75% of your plate should be from plant produce in some capacity.
Vegetables (broccoli, cabbage, cucumber, bell pepper, spinach, green beans, okra, celery, arugula, etc.)
Eat enough protein. Amounts are unique to the individual, but generally speaking, MOST people need at least 20-30 grams of protein per meal (totaling at least 80-100 grams per day). More specifically, this should be derived from ANIMAL sources like eggs, meat, fish. Gut lining integrity is highly dependent on amino acid delivery to support enterocyte and colonocyte recycling. This is dependent on amino acids— namely glutamine. Glutamine is a conditionally essential amino acid which means that our body is capable of producing it, but during times of high demand (like when there is gut inflammation and stress resulting in high cell turnover), glutamine becomes essential in the diet (meaning we have to consume it to meet demands). Glutamine is most abundant and bioavailable in animal-derived proteins including meat, organs, seafood, eggs, and bone broth.
Support proper “meal time hygiene”
Limiting Distractions
Giving yourself ample Duration
Enhance Digestibility of foods… especially during periods of stress
Downtime between meals. This allows the MMC (migrating motor complex) to do its work! The migrating motor complex (MMC) is a cyclic, recurring motility pattern that occurs in the stomach and small bowel during fasting and it is interrupted by feeding. Think of it like a big wave-like motion that rushes over the entire intestinal tract between meals to clear out debris and reset the immune system. Its absence has been associated with gastroparesis, intestinal pseudo-obstruction and small intestinal bacterial overgrowth.
3. Include probiotic rich foods like sauerkraut or kimchi as well as prebiotic foods (vegetables, nuts, seeds, beans, etc.)! Probiotic supplementation can be helpful, but is pretty unique to the individual. For those with slow motility and intestinal bacterial overgrowth, sometimes probiotics can make the situation worse!
4. Make sure you’re pooping at least 1 time per day. This is a BIG one. The bowels are the largest means of detoxification in the body. When you’re not pooping at least once per day, stool sits inside your colon which is a big re-absorption organ. This is great for reabsorption of electrolytes and fluids, but not so great when your body is trying to also get rid of toxins (including bacterial byproducts, toxic byproducts of metabolism, bound hormones ready for excretion, and environmental toxins that we’re inevitably exposed to).
5. If you’re having persistent gut issues and you’re doing ALL THE THINGS, it may be time to work with a pro. Reach out if you think you need extra help! I am an advocate of having a medical doctor, specifically a gastroenterologist, on your team for medical management and diagnostics in addition to a support system, like a Dietitian, to help personalize a dietary strategy for you!
References:
Bargiel P, Szczuko M, Stachowska L, Prowans P, Czapla N, Markowska M, Petriczko J, Kledzik J, Jędrzejczyk-Kledzik A, Palma J, Zabielska P, Maciejewska-Markiewicz D. Microbiome Metabolites and Thyroid Dysfunction. Journal of Clinical Medicine. 2021; 10(16):3609. https://doi.org/10.3390/jcm10163609
Patil AD. Link between hypothyroidism and small intestinal bacterial overgrowth. Indian J Endocrinol Metab. 2014 May;18(3):307-9. doi: 10.4103/2230-8210.131155. PMID: 24944923; PMCID: PMC4056127.
Ramezani M, Sajadi Hezaveh Z. The effect of synbiotic supplementation on thyroid hormones, blood pressure, depression and quality of life in hypothyroid patients: A study protocol for a randomized double-blind placebo controlled clinical trial. Clin Nutr ESPEN. 2022 Apr;48:472-478. doi: 10.1016/j.clnesp.2022.01.003. Epub 2022 Jan 10. PMID: 35331531.
Daher R, Yazbeck T, Jaoude JB, Abboud B. Consequences of dysthyroidism on the digestive tract and viscera. World J Gastroenterol. 2009 Jun 21;15(23):2834-8. doi: 10.3748/wjg.15.2834. PMID: 19533804; PMCID: PMC2699000.
Docimo G, Cangiano A, Romano RM, Pignatelli MF, Offi C, Paglionico VA, Galdiero M, Donnarumma G, Nigro V, Esposito D, Rotondi M, Candela G, Pasquali D. The Human Microbiota in Endocrinology: Implications for Pathophysiology, Treatment, and Prognosis in Thyroid Diseases. Front Endocrinol (Lausanne). 2020 Dec 4;11:586529. doi: 10.3389/fendo.2020.586529. PMID: 33343507; PMCID: PMC7746874.
Fernández-García V, González-Ramos S, Martín-Sanz P, Laparra JM, Boscá L. Beyond classic concepts in thyroid homeostasis: Immune system and microbiota. Mol Cell Endocrinol. 2021 Aug 1;533:111333. doi: 10.1016/j.mce.2021.111333. Epub 2021 May 25. PMID: 34048865.
Knezevic J, Starchl C, Tmava Berisha A, Amrein K. Thyroid-Gut-Axis: How Does the Microbiota Influence Thyroid Function? Nutrients. 2020 Jun 12;12(6):1769. doi: 10.3390/nu12061769. PMID: 32545596; PMCID: PMC7353203.
Ruscio M, Guard G, Piedrahita G, D’Adamo CR. The Relationship between Gastrointestinal Health, Micronutrient Concentrations, and Autoimmunity: A Focus on the Thyroid. Nutrients. 2022 Aug 30;14(17):3572. doi: 10.3390/nu14173572. PMID: 36079838; PMCID: PMC9460308.
Fenneman AC, Bruinstroop E, Nieuwdorp M, van der Spek AH, Boelen A. A Comprehensive Review of Thyroid Hormone Metabolism in the Gut and Its Clinical Implications. Thyroid. 2023 Jan;33(1):32-44. doi: 10.1089/thy.2022.0491. Epub 2023 Jan 6. PMID: 36322786.
Gong B, Wang C, Meng F, Wang H, Song B, Yang Y, Shan Z. Association Between Gut Microbiota and Autoimmune Thyroid Disease: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne). 2021 Nov 17;12:774362. doi: 10.3389/fendo.2021.774362. PMID: 34867823; PMCID: PMC8635774.
Cayres LCF, de Salis LVV, Rodrigues GSP, Lengert AVH, Biondi APC, Sargentini LDB, Brisotti JL, Gomes E, de Oliveira GLV. Detection of Alterations in the Gut Microbiota and Intestinal Permeability in Patients With Hashimoto Thyroiditis. Front Immunol. 2021 Mar 5;12:579140. doi: 10.3389/fimmu.2021.579140. PMID: 33746942; PMCID: PMC7973118.
Rinninella E, Raoul P, Cintoni M, Franceschi F, Miggiano GAD, Gasbarrini A, Mele MC. What is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases. Microorganisms. 2019 Jan 10;7(1):14. doi: 10.3390/microorganisms7010014. PMID: 30634578; PMCID: PMC6351938.
Jung SJ, Kang JH, Roberts AL, et al. Posttraumatic stress disorder and incidence of thyroid dysfunction in women. Psychological Medicine. 2019;49(15):2551-2560. doi:10.1017/S0033291718003495
María L. Vélez, Eugenia Costamagna, Edna T. Kimura, Laura Fozzatti, Claudia G. Pellizas, María M. Montesinos, Ariel M. Lucero, Aldo H. Coleoni, Pilar Santisteban, Ana M. Masini-Repiso, Bacterial Lipopolysaccharide Stimulates the Thyrotropin-Dependent Thyroglobulin Gene Expression at the Transcriptional Level by Involving the Transcription Factors Thyroid Transcription Factor-1 and Paired Box Domain Transcription Factor 8, Endocrinology, Volume 147, Issue 7, 1 July 2006, Pages 3260–3275, https://doi.org/10.1210/en.2005-0789
Deloose E, Janssen P, Depoortere I, Tack J. The migrating motor complex: control mechanisms and its role in health and disease. Nat Rev Gastroenterol Hepatol. 2012 Mar 27;9(5):271-85. doi: 10.1038/nrgastro.2012.57. PMID: 22450306.
Sabatino L, Vassalle C, Del Seppia C, Iervasi G. Deiodinases and the Three Types of Thyroid Hormone Deiodination Reactions. Endocrinol Metab (Seoul). 2021 Oct;36(5):952-964. doi: 10.3803/EnM.2021.1198. Epub 2021 Oct 21. PMID: 34674502; PMCID: PMC8566136.
Ramamoorthy S, Cidlowski JA. Corticosteroids: Mechanisms of Action in Health and Disease. Rheum Dis Clin North Am. 2016 Feb;42(1):15-31, vii. doi: 10.1016/j.rdc.2015.08.002. PMID: 26611548; PMCID: PMC4662771.
Mincer DL, Jialal I. Hashimoto Thyroiditis. [Updated 2022 Jun 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459262/
Sinha RA, Bruinstroop E, Singh BK, Yen PM. Nonalcoholic Fatty Liver Disease and Hypercholesterolemia: Roles of Thyroid Hormones, Metabolites, and Agonists. Thyroid. 2019 Sep;29(9):1173-1191. doi: 10.1089/thy.2018.0664. PMID: 31389309; PMCID: PMC6850905.
Agha-Hosseini F, Shirzad N, Moosavi MS. Evaluation of Xerostomia and salivary flow rate in Hashimoto’s Thyroiditis. Med Oral Patol Oral Cir Bucal. 2016 Jan 1;21(1):e1-5. doi: 10.4317/medoral.20559. PMID: 26595829; PMCID: PMC4765761.
Disclaimer: Please note that “Thyroid School” emails and blogs from and written by Chews Food Wisely, LLC (and Nicole Fennell, RD) are not intended to create any physician-patient relationship or supplant any in-person medical consultation or examination. Always seek the advice of a trained health professional with any questions you may have regarding a medical condition and before seeking any treatment. Proper medical attention should always be sought for specific ailments. Never disregard professional medical advice or delay in seeking medical treatment due to information obtained in “Thyroid School” emails. Any information received from these emails is not intended to diagnose, treat, or cure. These emails, websites, and social media accounts are for information and educational purposes only. The information in these emails, websites, and social media accounts is not intended to replace proper medical care.
Nicole Fennell is a functional nutrition Dietitian—and a fellow Hashimoto’s patient—who understands firsthand the challenges of living with thyroid hormone imbalances and immune system dysfunction. Her approach to managing chronic disease and stubborn symptoms focuses on building the body up with enjoyable and realistic nourishment rather than breaking it down with restrictive, unrealistic, short-term diets.
With a real-food philosophy, Nicole emphasizes the power of nutrition, movement, and peace of mind in both disease prevention and long-term health. Outside of her work, she loves staying active with her husband and three kids, lifting weights, practicing yoga, walking, cooking, enjoying good food, and spending time outdoors.
free resources
Want to kickstart your journey without feeling overwhelmed? Checkout our free thyroid warrior resources to feel empowered as you navigate your health journey
Whether you’re dealing with exhaustion that never ends, a Hashimoto's diagnosis, thyroid issues, hormone imbalances, painful PMS, or stubborn acne that just won’t quit—please know you’re not alone. At Chews Food Wisely, we’re all about connecting the dots between your never ending list of symptoms and personalized nutrition solutions that last.